What is revision rhinoplasty?
Revision (secondary) rhinoplasty is performed to correct aesthetic and/or functional problems that persist or develop after a previous nose surgery. It is generally more complex than primary rhinoplasty due to scar tissue, weakened cartilage support, and altered anatomy. The goal is to achieve better facial harmony, restore structural support, and improve breathing function in suitable patients.
Revision rhinoplasty rates after primary surgery are reported in international literature at approximately 5-15%. This rate varies with surgical technique, patient anatomy, skin type, and individual healing. The need for revision does not necessarily indicate a "mistake" in the first surgery — it can result from natural healing variability.
Who is a candidate?
Candidates include patients dissatisfied with previous rhinoplasty results, those with tip drooping, asymmetry, bridge irregularities, breathing difficulties, or structural issues after first surgery.
A minimum of 12 months after the initial surgery is typically recommended for revision planning — sufficient time for swelling and scar maturation. Revisions before 12 months can lead to misleading planning. In some complex cases, 18-24 months of waiting is preferred — particularly for thick-skinned patients in whom tip swelling resolves slowly.
How is the approach determined?
Each revision is individually planned based on the current nasal structure. Cartilage grafts (from septum, ear, or rib) may be necessary. Both open and closed techniques can be used depending on the complexity of the case.
Septal cartilage: First-choice graft source if not exhausted in the prior surgery. Provides natural-feeling support.
Auricular (ear) cartilage: Used for tip support and alar batten grafts. Curved by nature, advantageous in some applications. Postauricular incision is virtually invisible.
Costal (rib) cartilage: Gold standard for complex revisions. Harvested through a 3-4 cm incision at the 6th or 7th rib. Provides abundant, strong, straight or shapeable grafts. Preferred for saddle nose deformity, large collapse defects, and advanced tip reconstruction.
Preoperative preparation
Smoking should be stopped at least 4 weeks before surgery. Smoking impairs already-compromised nasal skin microcirculation; tissue healing risks are markedly higher in revision cases compared to primary surgery.
Previous operative notes, available pre/post photos, and prior imaging should be brought to consultation. Information about the technique used and grafts placed previously is critical for surgical planning. International patients are asked to share these documents during video consultation prior to travel.
Standard preoperative tests, plus paranasal sinus CT for revision cases — to evaluate internal anatomy, septal status, and previous graft positions.
The surgery
Revision rhinoplasty is performed under general anesthesia in an accredited hospital. Surgery time is generally longer than primary (2-4 hours); complex cases involving rib cartilage harvest may extend to 5 hours. Hospital stay is 1 night.
Open technique is most often preferred in revision cases for the wide visualization and precise structural correction. Postoperatively a thermoplastic splint is placed; removed at day 7. Internal splints, if used, are removed at days 5-7.
Recovery timeline
First week: Swelling and bruising are typically more pronounced than primary. Splint and stents removed at day 7.
Weeks 2-4: Gradual return to social activities. Swelling persists especially at the tip.
Months 1-3: 60-70% of swelling resolves. Structural result emerges.
1-2 years: Final result settles later than primary cases. Scar tissue delays swelling resolution; in thick-skinned patients, up to 2 years may be needed. Regular follow-up during this period is essential.
Risks and complications
Revision rhinoplasty carries higher risk than primary rhinoplasty. Scar tissue, anatomical disruption, and reduced graft sources reduce surgical predictability.
Early-period: Bleeding, infection, tissue healing problems (markedly higher in smokers), graft displacement.
Late-period: Graft resorption, asymmetry, weakened tip support, functional valve issues. Graft warping is a recognized late complication of rib cartilage; minimized with modern techniques.
Need for additional revision: The rate of further revision after revision rhinoplasty is reported in international literature at 10-20%. Patients should be informed of this possibility.
Revision rhinoplasty in Istanbul — Assoc. Prof. Dr. Ayhan Işık Erdal's practice
Dr. Erdal's private clinic is located in central Istanbul, in the Nisantasi district. Address: Teşvikiye Cad. No:9/12, Istanbul. The clinic is easily accessible from major Istanbul hotels and from Istanbul Airport (IST) and Sabiha Gökçen Airport (SAW).
Revision rhinoplasty is regarded as one of plastic surgery's most demanding procedures; experience, technical knowledge, and anatomical insight are critical. Patients dissatisfied with prior rhinoplasty results tend to be even more selective in choosing their second surgeon. Istanbul has emerged as a leading destination for revision rhinoplasty, attracting patients from Europe, North America, the Middle East, and Asia for board-certified surgeons specializing in revision cases, accredited hospitals, competitive pricing, and structured medical tourism support.
Dr. Erdal's Istanbul practice provides extended consultation time for revision cases. Previous operative photos, current anatomical state, patient goals, and realistic expectations are evaluated in detail. Preoperative imaging (sinus CT) analyzes the existing structure. For cases planned to use rib cartilage, patients are also informed about donor site healing. International patient coordination includes video consultation prior to travel, airport-hotel transfer, English-speaking medical team, accommodation at partner hotels, and full postoperative follow-up. Patients typically stay in Istanbul for 7-10 days following revision rhinoplasty. WhatsApp consultations are available at +90 544 850 72 32 for international inquiries.
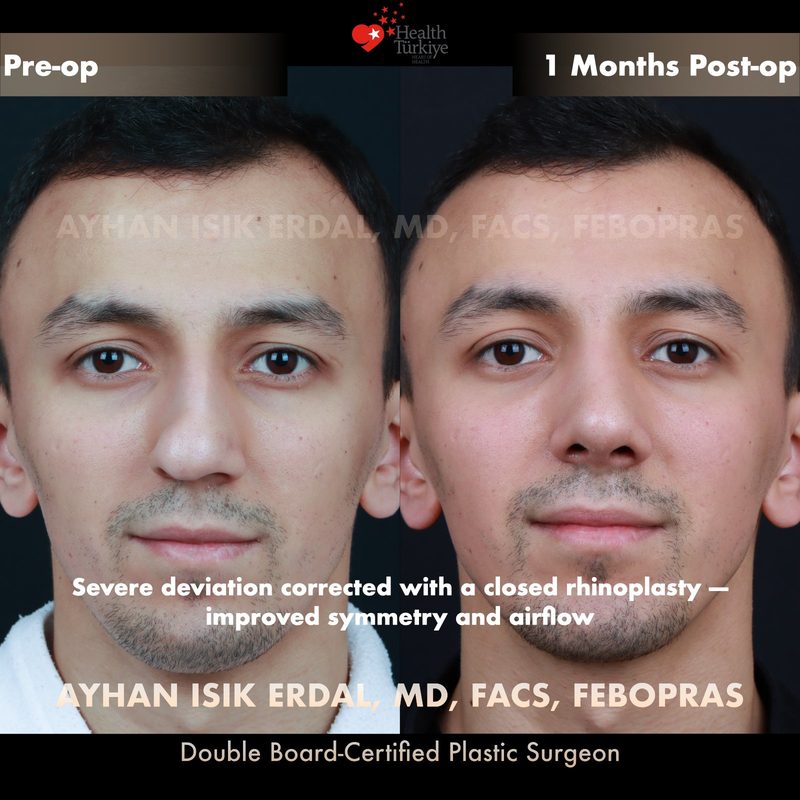
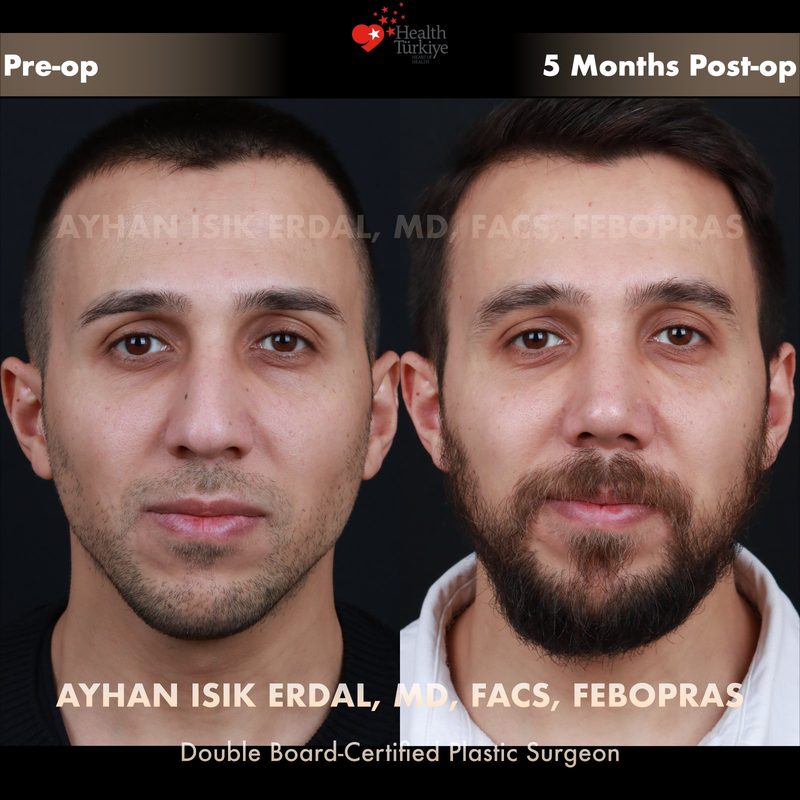
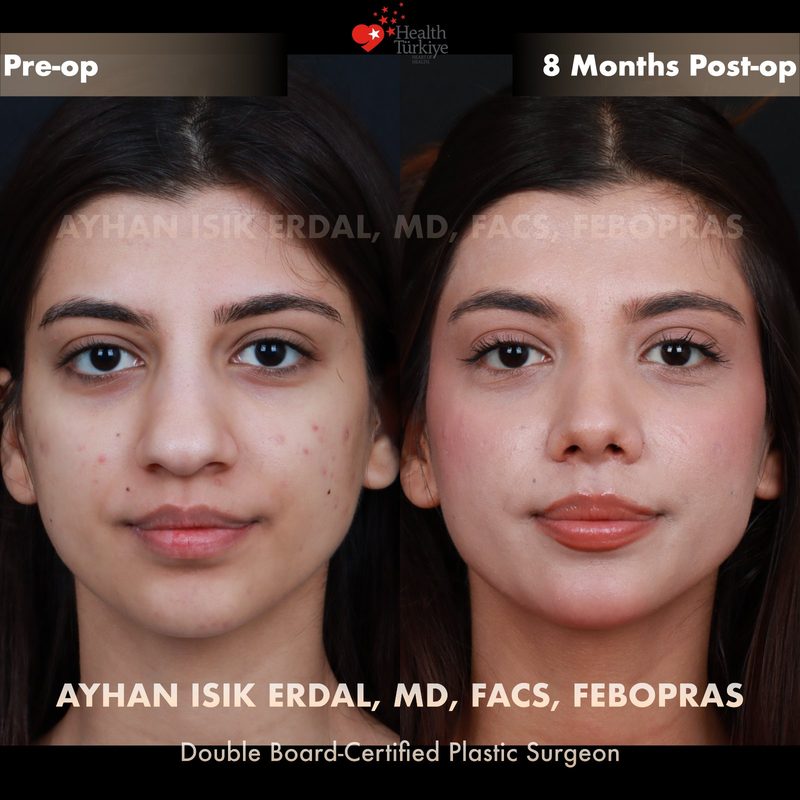
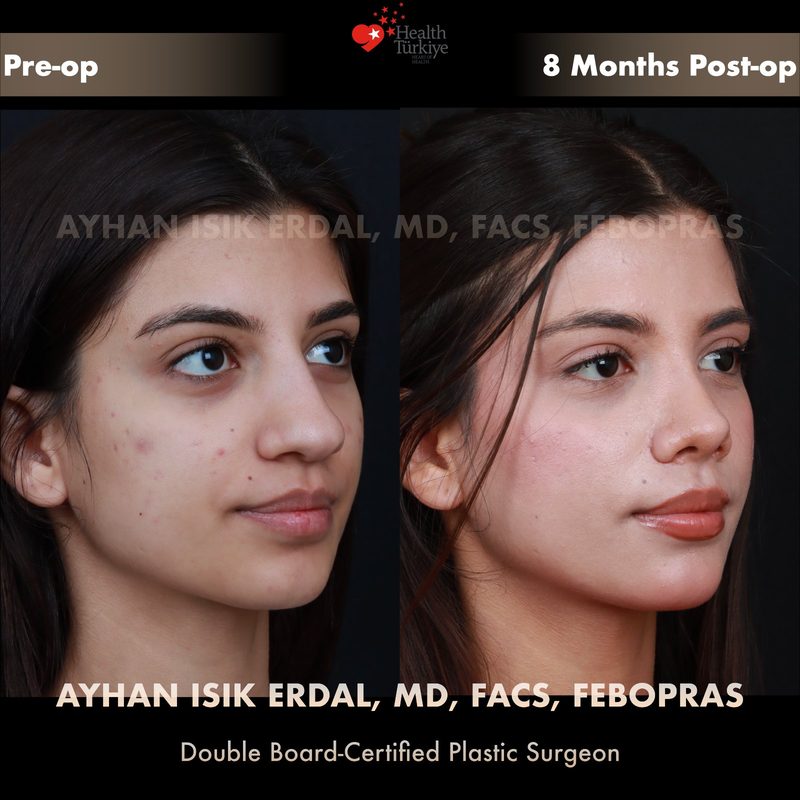
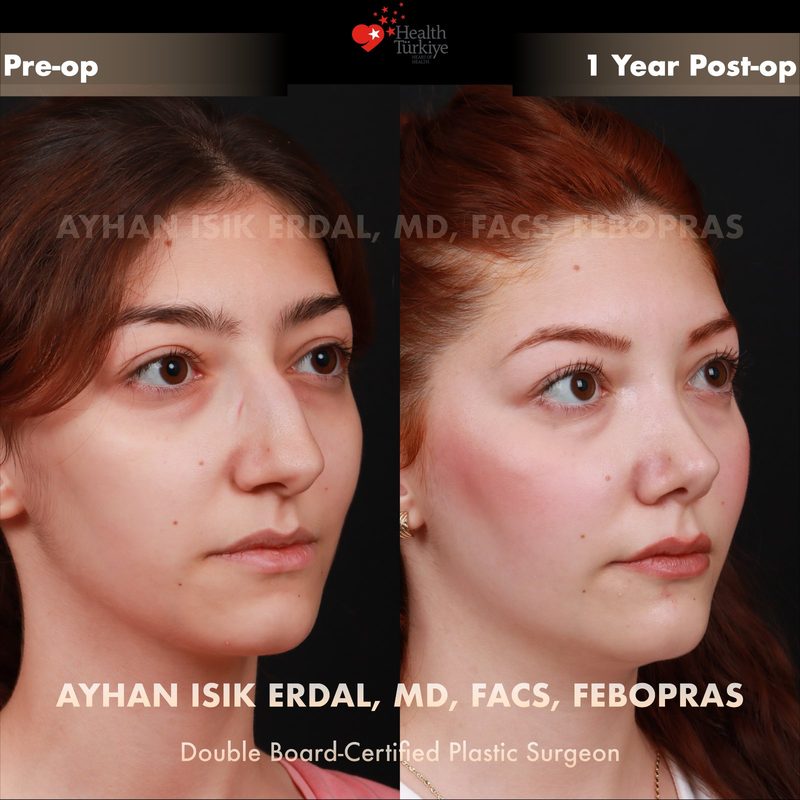
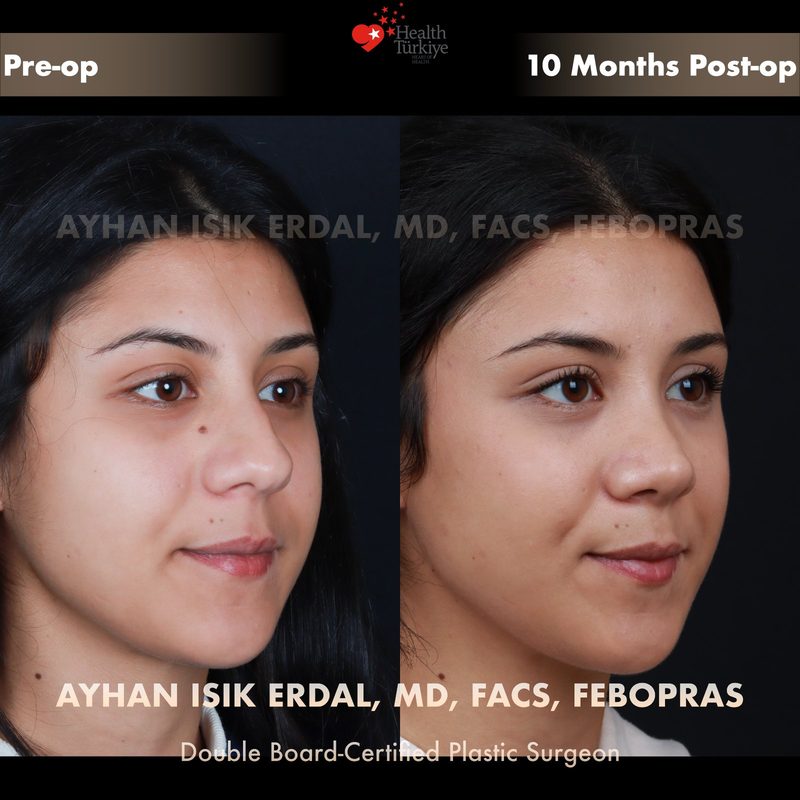
Before & After Gallery — Rhinoplasty
Real patient results. Photos shared with patient consent. Individual results may vary.











































Frequently Asked Questions
Generally yes, due to scar tissue, reduced cartilage, and altered anatomy. Careful planning is essential.
At least 12 months after the initial surgery to allow full healing and scar maturation.
Pain levels are generally similar to primary rhinoplasty. If rib cartilage grafting is needed, there may be additional discomfort at the donor site.
If septal cartilage was used in the first surgery or is insufficient, rib cartilage provides the strongest and most abundant graft material for structural reconstruction.
In experienced hands, revision rhinoplasty achieves high satisfaction rates. However, each case is unique and results depend on the current nasal condition. Realistic expectations are important.
Technically possible, but each revision is more complex than the last. Tissue quality decreases with each surgery, making the first revision critically important.
Overall recovery is similar, but swelling may resolve slightly slower due to scar tissue, particularly at the tip.
Yes. Breathing difficulties, septal deviation, and valve collapse can be addressed during revision surgery. Aesthetic and functional correction is typically combined.
If after 12+ months you have persistent aesthetic concerns, breathing difficulties, or structural issues that developed over time, a revision consultation is appropriate.
If functional issues are documented (breathing obstruction), some insurance plans may cover the functional component. Coverage varies by country and policy.
Book a Consultation
For more information about Revision Rhinoplasty and to schedule a consultation, please get in touch.
WhatsApp